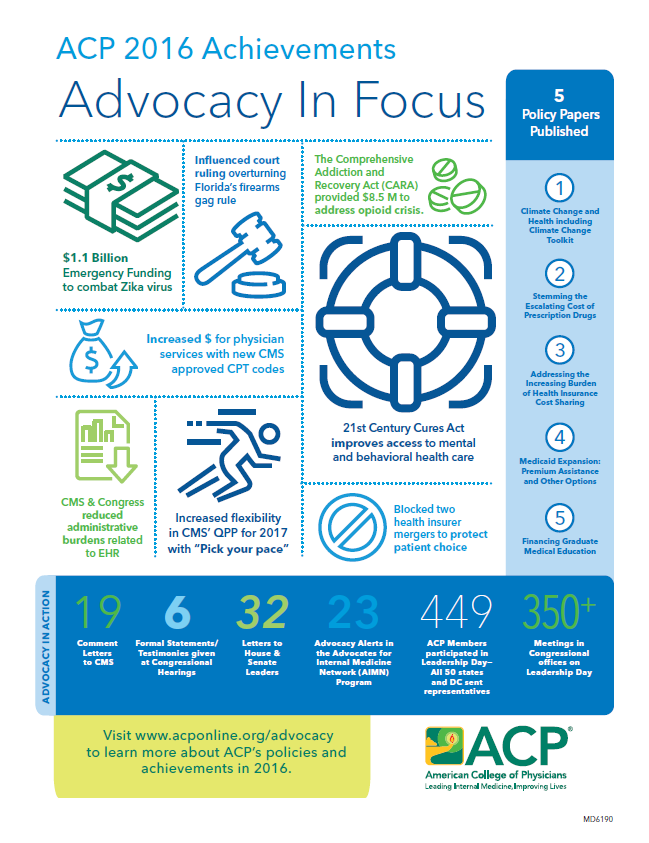
What ACP Advocacy Did For You and Your Patients in 2016
Over the past year, ACP was successful in advancing significant policy reforms on behalf of internal medicine physicians, related subspecialists, and their patients.
These achievements were the result of considerable effort, not only on the part of ACP, but also in collaboration with other allied organizations and coalitions, in both the legislative and regulatory spheres.
- Increased payments for physicians services
- Curbed harm from health insurer consolidations
- Reduced administrative burdens
- Improved practice environment with more flexibility and options
- Helped patients access vital care and treatment
- Influenced court ruling overturning Florida's firearms gag rule
Increased payments for physicians services
Because of ACP advocacy, Medicare will now reimburse physicians for a series of new CPT codes in the areas of chronic care management, non-face-to-face prolonged services, behavior health integration and psychiatric care. This will enable physicians to bill Medicare for services that previously would not have been covered. In many instances, physicians have already been providing such services – in varying degrees – to their patients without being justly compensated so these new codes represent a big step forward in recognizing the time they devote to their patients.
ACP advocated with the Centers for Medicare and Medicaid Services (CMS) to authorize payment for certain services that were not being covered or even recognized by Medicare; in some cases these were services already being provided to patients by physicians and yet they still could not bill or be reimbursed for them. Because of ACP advocacy, CMS subsequently agreed to allow payment for the following new services and codes:
- Complex Chronic Care Management (CCM): Complex CCM codes that promote care of patients with chronic illnesses – specifically, for CCM services that extend to 60 minutes in length.
- Non-Face-to-Face Prolonged Services: CPT codes for non-face-to-face prolonged E/M services by the physician (or other billing clinician) that are currently bundled, and increased payment rates for face-to-face prolonged E/M services by the physician (or other billing clinician) based on existing Relative Value Scale Update Committee (RUC) recommended values.
- Care Management Services for Behavioral Health Conditions (G0507): A G-code that describes care management for beneficiaries with diagnosed behavioral health conditions under a broader application of integration in the primary care setting; at least 20 minutes of clinical staff time, directed by a physician or other qualified health care professional time, per calendar month, for collaborative care and care management for beneficiaries with behavioral health conditions.
- Initial Psychiatric Collaborative Care Management (G0502): A G-code for the first 70 minutes in the first calendar month of behavioral health care manager activities, in consultation with a psychiatric consultant, and directed by the treating physician or other qualified health care professional.
- Subsequent Psychiatric Collaborative Care Management (G0503): A G-code in the first 60 minutes in a subsequent month of behavioral health care manager activities, in consultation with a psychiatric consultant, and directed by the treating physician or other qualified health care professional.
- Initial or subsequent psychiatric collaborative care management (G0504): A G-code for each additional 30 minutes in a calendar month of behavioral health care manager activities, in consultation with a psychiatric consultant, and directed by the treating physician or other qualified health care professional.
Curbed harm from health insurer consolidations
Because of ACP advocacy, federal judges blocked two separate health insurer mergers that would have resulted in decreased choice of health plans and increased costs for patients and employers; had the mergers been approved, the merged companies would have been able to impose narrow networks that would reduce patient access to physicians and hospitals and dictate contract terms to physicians, effectively preventing physicians from negotiating over provisions of health services with those insurers. The courts ruled against the mergers on the basis that they would result in a stifling of competition in the market and less consumer choice—as ACP argued. While subject to appeal, these rulings represent significant wins for consumers and employers alike and ACP applauded the decisions.
In 2016, ACP sent letters to the U.S. Department of Justice and aggressively advocated to oppose the mergers of Aetna and Humana and also Anthem and Cigna. On Jan. 23, 2017, a federal judge blocked Aetna’s merger with Humana after finding that the health insurers’ $37 billion deal would leave seniors with fewer and costlier options for private Medicare coverage. The merger risked irreparably harming competition within the Medicare Advantage market, and would hand Aetna and Humana a near monopoly across the nation, wrote U.S. District Court Judge John D. Bates in a verdict issued that day. A similar ruling came down from a federal judge on Feb. 8, 2017 blocking a proposed $54 billion deal for Anthem to acquire Cigna.
Reduced administrative burdens
While ACP is committed to pushing for even more relief for physicians from unnecessary paperwork and documentation requirements, much progress was made in 2016 to reduce administrative burdens in the EHR Meaningful Use Program and in the reporting of chronic care management services, but also advancements to develop interoperability standards and the sharing of patient data, as permissible under law. Much of ACP’s advocacy on reducing administrative burdens on physicians has centered on health information technology (Health IT) and the myriad of federal regulatory and administrative requirements placed on physicians and others who must operate this technology. Electronic Health Records (EHRs) lack standards that are needed for systems to be able to talk to each other in a way that is meaningful. In many instances, physicians are required to input data into these records that have little to no clinical value. The costs associated with the systems that support EHRs can be exorbitant. And, there is a need for EHR developers and vendors to do more to improve the usability, functionality, and interoperability of their products. Physicians contend with these hassles on a daily basis but 2016 brought some marked improvements in this area.
Through a series of comment letters to CMS and to Congress, as well as direct person-to-person member advocacy through Leadership Day, ACP aggressively pushed for some much-needed improvements to EHR interoperability and usability and brought attention to some unanticipated administrative burdens associated with some CPT codes. ACP subsequently applauded actions taken by Congress through enacted legislation or CMS through the rulemaking process to reduce administrative burdens, including:
- Meaningful Use of EHRs: CMS shortened the reporting period for MU in calendar year (CY) 2016 from the full CY to any continuous 90-day period; adding policy on measure calculations that fall outside of the 90-day reporting period; and updating reporting requirements for eligible professionals (EPs) that are new participants in the program in 2017 as well as offering a one-time significant hardship exception for these new participants.
- EHR Interoperability Standards: Enacted into law, the 21st Century Cures Act created a Health IT Advisory Committee, which must analyze existing standards, including an evaluation of the need for a core set of common data elements and associated value sets to enhance the ability of certified health information technology to capture, use, and exchange structured electronic health information.
- “Information Blocking”: The 21st Century Cures Act made improvements to address the practice of interfering with the ability to share patient data whenever permitted by law, known as “information blocking.” The Secretary of Health and Human Services shall make a requirement of certification that health IT developers: do not block information; do not prohibit or restrict communication regarding usability, interoperability, security, user experience, business practices of developers, and how users use health IT. The Secretary must also identify reasonable and necessary activities that do not constitute information blocking.
- Chronic Care Management Codes (CCM): With the initial implementation of CCM codes in 2015, which ACP welcomed, ACP had expressed concern about administrative burdens associated with reporting CCM services. CMS recognized through comments from numerous professional societies (including ACP), and underutilization of the codes, that some of the service elements and billing requirements were too burdensome and they proposed a number of changes to the current elements required to provide and bill CCM services including: requirements for the initiating visit; 24/7 access to care and continuity of care; format and sharing of the care plan and clinical summaries; beneficiary receipt of the care plan; beneficiary consent; and documentation.
- Strategies for Reducing Burden: The 21st Century Cures Act required the Secretary to develop a strategy and recommendations to meet the goal of reducing regulatory or administrative burdens (such as documentation requirements) relating to the use of EHRs. The strategy should include: examining incentive programs for Medicaid, MIPS, APMs, and Hospital Value Based Purchasing; EHR certification requirements, standards and implementation specifics, activities related to security of and patients access to electronic information, health and clinical research, public health, reporting clinical data for administrative reasons and aligning and simplifying quality measures across Federal programs and other payers.
Improved practice environment with more flexibility and options
With the elimination of Medicare’s physician payment system, the Sustainable Growth Rate (SGR), in 2015 and its subsequent replacement to a new payment and delivery system under the Medicare Access and CHIP Reauthorization Act (MACRA), now the Quality Payment Program (QPP), physicians had to begin preparing in 2016 for major changes to their practice environments. The roll-out of MACRA and other CMS payment model initiatives in 2016 meant practices had to learn how to navigate under these new reforms, which will continue to unfold in years to come. Physicians had to reassess their practice environment, determine what payment structure best fit their needs, either under an alternative payment model (APM) or the Merit-based Incentive Payment System (MIPS). CMS also unveiled new, expanded initiatives that brought opportunity to practices, like through the Comprehensive Primary Care + Program, in which ACP actively urged its member practices in eligible states to participate. Unlike the days of the strict SGR payment formula where physicians only saw a one-sized fits all approach to payments that brought with it yearly threats of significant payment cuts, 2016 ushered in these new value-based payment systems that offer physicians and their practices more choice, control, and flexibility.
“Pick Your Pace”: As advocated by ACP, in October 2016, CMS finalized regulations implementing the QPP, and included some much-needed flexibility to practices in when they transition to QPP. “Pick your Pace,” as it is known, allows physicians to choose from among four options in which to transition to QPP based on what works best for them and their practices. As long as physicians choose one of the four options, they will be protected from negative adjustments in 2019 and even have the opportunity for positive adjustments.
Critical Improvements under the MIPS Pathway: Physicians will be able to choose between two payment pathways under the new Quality Payment Program (QPP), either the MIPS or APM pathway, depending on their practice structure. Most physicians will fall under MIPS during the first payment year, which begins in 2019 (based on performance in 2017). MIPS essentially streamlines existing Medicare quality programs including the Physician Quality Reporting Program (PQRS), the Value-Based Payment Modifier (VM), and the Medicare EHR Incentive Program (MU) into one program. Physician payments under MIPS will be based on a composite score using four weighted performance categories [Quality at 60% + Advancing Care Information/(i.e. EHRs) at 25% + Improvement Activities (i.e. clinical) at 15% + Cost (i.e. resource use) at 0]. Thanks to ACP advocacy, CMS incorporated into the final QPP regulations our recommendations to simplify and reduce burdens on physicians and their practices. These included:
- MIPS Scoring/Cost: ACP successfully advocated for CMS to eliminate inaccurate measures of physicians’ cost of care in the 2017 performance year to determine updates on the MIPS program. Originally, 10% of physicians’ performance update would have been based on cost of care; because of ACP advocacy, cost of care was completely removed as a factor in 2017, instead being moved into the quality category. ACP argued this adjustment to the weighting was needed in the first year because the cost measures had not proven to be reliable, validated measures in their application to physicians.
- MIPS Scoring/Quality: Rather than the more onerous policies under the Physician Quality Reporting System (PQRS), which required physicians to report on 9 quality measures across at least 3 National Quality Strategy (NQS) domains, CMS reduced the number of measures required to 6 quality measures and eliminated the requirement to report in multiple NQS domains.
- Small Practices under MIPS: The low-volume threshold for participation in MIPS was raised to less than $30,000 in Medicare Fee-for-Service (FFS) revenue OR less than or equal to 100 Medicare patients, which will help provide a better safety net for small practices. This was significant because the MACRA law requires CMS to set a low-volume threshold at which clinicians who fall below are not considered eligible clinicians for the purposes of MIPS. CMS had originally proposed to define MIPS eligible clinicians or groups who do not exceed the low-volume threshold as those who have Medicare billing charges of less than or equal to $10,000 AND provide care for 100 or fewer Part B-enrolled beneficiaries during the performance period. Thanks to ACP’s advocacy, CMS later modified the low-volume threshold to include ECs and groups with $30,000 in Part B allowed charges OR 100 or fewer Part B patients. This will help provide a better safety net for small practices and certain specialists/subspecialists with a small Medicare patient population.
- Patient Centered Medicare Homes under MIPS: CMS agreed to broaden its definition of the patient centered medical home and comparable specialty practices for the purposes of full improvement activities credit to specifically be inclusive of programs that have a demonstrated track record of support by non-Medicare payers, state Medicaid programs, employers, and/or others in a region or state. The MACRA law specifies that a MIPS eligible clinician or group that is certified as a patient- centered medical home (PCMH) or comparable specialty practice with respect to a performance period must be given the highest potential score for the improvement activities performance category. CMS has defined a PCMH for the purposes of full credit within this category as one that “is a nationally recognized accredited patient-centered medical home, a Medicaid Medical Home Model, or a Medical Home Model.” CMS finalized its regulation stating a MIPS eligible clinician or group as being a certified patient-centered medical home or comparable specialty practice if they have achieved certification or accreditation as such from a national program. The Agency expanded this definition to also include a regional or state program, private payer or other body that administers patient-centered medical home accreditation and certifies 500 or more practices for patient-centered medical home accreditation or comparable specialty practice certification. This means that more practices would qualify to earn full credit in the improvement activities category through participation in a PCMH program.
The Comprehensive Primary Care Plus (CPC+) Model: In April 2016, CMS unveiled the CPC+, which is a national advanced primary care medical home model that aims to strengthen primary care through regionally-based multi-payer payment reform and care delivery transformation. CPC+ is a five-year model, to begin in January 2017, that includes two primary care practice tracks with incrementally advanced care delivery requirements and payment options. Come 2017, it will support nearly 5,000 primary care practices in 20 regions, and serve millions of Medicare beneficiaries. ACP applauded the CPC+, and further advocated that CMS allow participating clinicians in the CPC+ to also participate in the Medicare Shared Savings Program (MSSP), which consists of groups of doctors and other health care providers who band together under Accountable Care Organizations (ACOs) and voluntarily work together with Medicare to improve the quality of care to Medicare Fee-for-Service beneficiaries and reduce unnecessary costs. Thanks to ACP advocacy, CMS agreed to allow dual participation by primary care practices in CPC+ and MSSP. In addition, new participants in CPC+ would be considered Advanced APMs for the 2018 performance period under QPP. And, since CPC+ participating practices must have enhanced capabilities such as those that promote access, care management, comprehensive care and care coordination, and patient engagement, this affords practices care management payments and performance incentives based on the enhanced care offered to patients.
Helped patients access vital care and treatment
Through a series of bipartisan bills, legislation was enacted to improve access to care, and treatment for those suffering from mental and behavioral health conditions, opioid addiction, and the Zika virus, a mosquito-borne virus that grew to epidemic proportions in 2016 and ravaged populations around the globe. Enacted legislation included vital funding for research, initiated and expanded grant programs for treatment for these afflictions, and increased awareness as to the enormous toll of these conditions on the nation’s public health. ACP’s advocacy included active engagement with Congress to advance these measures. Physicians continue to be on the front lines in caring for many patients who present with these afflictions. Thanks to much-needed reforms in 2016, their patients will see greater access to care and treatment for these conditions.
ACP actively engaged Congress, through letters, meetings, and coalition efforts to educate lawmakers about the growing need to address the opioid crisis, improve access to mental and behavioral health services (especially in the primary care setting), and fund research efforts to stem the spread of the Zika virus. This prompted congressional action and subsequent progress was made in addressing these issues through legislation that was enacted into law.
- Preventing and Treating Opioid Use Disorders: The Comprehensive Addiction and Recovery Act (CARA), in tandem with the 21st Century Cures Act, provided $8.5 million in funding to combat opioid use, along with a myriad of federal and state grant programs designed to address the growing crisis of opioid addiction.
- Improving Access to Mental and Behavioral Health: The 21st Century Cures Act included provisions to improve and increase access to treatment for patients suffering from mental health and substance use disorders and ensure better understanding and enforcement of mental health parity laws. It included alternatives to incarceration that divert individuals with mental illness from the criminal justice system to community-based treatment programs. It also will accelerate the integration of behavioral health into the primary care setting.
- Zika Virus: Congress enacted legislation that included $1.1 billion in emergency funding for the U.S. Department of Health and Human Services and the State Department/U.S. Agency for International Development to combat the Zika virus. ACP urged Congress to provide the highest possible funding level for research, prevention, control, and treatment of illnesses associated with the Zika virus that is commensurate with the public health emergency that the virus represents.
Influenced court ruling overturning Florida's firearms gag rule
In 2011, the state of Florida passed a law that restricted physicians' ability to discuss firearm safety with patients. Under its provisions, doctors could be punished with a fine of up to $10,000, and could lose their medical licenses for discussing firearms with patients. That Florida law violated physicians’ First Amendment rights and directly contradicted ACP’s long-standing policy that seeks to protect the doctor-patient relationship. Shortly thereafter, a group of individual physicians and medical specialty societies, including ACP’s Florida chapter, joined together to file a lawsuit against the state of Florida challenging this law. Known as Wollschlaeger v. State of Florida, or the “docs vs. glocks” case, ACP’s Florida chapter joined the local chapters of the American Academy of Pediatrics, American Academy of Family Physicians, and others in bringing this lawsuit against the state based on the contention that physicians should not be prohibited by law or regulation from discussing with or asking their patients about risk factors, or disclosing information to the patient, which may affect their health, the health of their families, sexual partners, and others who may be in contact with the patient. After several years of on-going advocacy and battling this out in the lower courts, the ACP Florida chapter and its co-plaintiffs emerged victorious when a federal court overturned the Florida law on Feb. 16, 2017. The national ACP joined in amicus curiae (“friend of the court”) briefs supporting the plaintiff’s case along the way. This represents a big achievement for ACP and for physicians who can now freely discuss with their patients ways to prevent injuries and deaths, including those associated with having unsecured firearms in their home. Since 2011, 14 other states have considered legislation similar to Florida’s, but none of the proposals have passed.
The Feb. 16 ruling of the United States Circuit Court of Appeals for the 11th Circuit said that doctors could not be threatened with losing their licenses for asking patients if they owned guns and for discussing gun safety because to do so would violate their free speech. ACP strongly opposed Florida’s Firearms Owners Privacy Act and joined eight other medical specialty societies in signing an Amicus Brief urging the U.S. Court of Appeals for the 11th Circuit to uphold a lower court decision that ruled the law unconstitutional. The plaintiffs, including the Florida Chapter of the American College of Physicians, individual Florida doctors, the Florida Pediatric Society/Florida Chapter of the American Academy of Pediatrics, and the American Academy of Family Physicians, Florida Chapter, sued the state of Florida for its unconstitutional intrusion on physicians’ constitutional right to speak freely to patients about the risk of unsecured firearms in the home; the national ACP joined in an amicus brief to the court supporting the plaintiff’s case.
A June 17, 2014 article published in the Annals of Internal Medicine said, it is estimated that each year, firearms kill more than 33,000 people in the United States. These deaths include homicides, suicides, and unintentional fatalities. The number of non-fatal firearm injuries in the United States is more than twice the number of fatal firearm injuries, with 73,883 non-fatal firearm injuries documented in 2011. ACP has long recommended that physicians ask about gun ownership as a normal part of screening patients, including it on a long list of health questions about drug and alcohol use, smoking, exercise and eating habits. The College believes that constitutional issues addressed by the court decision are much bigger than guns. It affirms a basic constitutional principle that the government should not be allowed to tell physicians what they can and can’t discuss with their patients, consistent with evidence-based standards of care.